
Baby spill on the shoulder is a badge of honour for new parents. But while some babies simply require piles of spit cloths, others —with extreme symptoms —may require medical intervention. Paediatrician Dr Anne Tait explains.
Gastro-oesophageal reflux (aka spilling or spitting) has been discussed in parenting circles since the beginning of time. It even gets a mention in Shakespeare’s famous speech from As You Like It: "All the world’s a stage... And one man in his time plays many parts, his acts being seven ages. At first the infant, mewling and puking in the nurse’s arms…" However, while commonplace, reflux and reflux-like conditions can still be a very traumatic introduction to parenthood.
It is important to know what is normal before we can define what is abnormal, and therefore explore treatment options. My approach to these issues is scientific and evidence-based, rather than anecdotal or opinion-based.
Spilling the facts
Gastro-oesophageal reflux (as opposed to gastro-oesophageal reflux disease) is a very normal physiological process for all people, at any age. Reflux is the movement of gastric contents into the oesophagus; spilling or vomiting is when those contents come out of the mouth. Reflux occurs in all adults after meals and lasts less than three minutes. Fifty percent of infants spill daily, this is totally normal. The reason why infants spill is due to a combination of factors, including having a liquid diet, being fed in a largely horizontal position, not yet being able to sit up and thus spending a lot of the time horizontal, and most importantly, the failure of the lower oesophageal sphincter to develop until the age of 6-12 months.
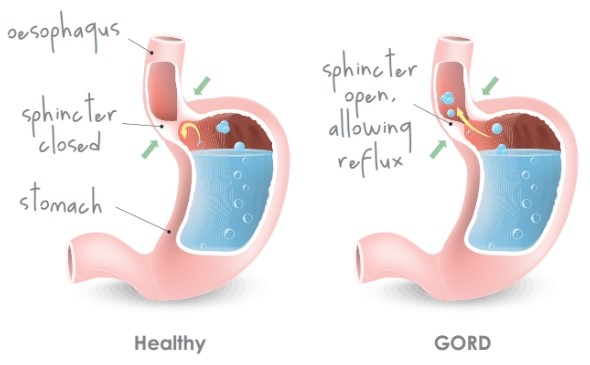
The lower oesophageal sphincter is a junction between the oesophagus and the top part of the stomach, and it prevents a large amount of gastric contents from refluxing up. As adults, we have all had the experience where we have eaten too much and we feel like we should vomit, however we cannot. The reason why we cannot vomit easily is because of our lower oesophageal sphincter being relatively tight. In adults, this lower oesophageal sphincter can loosen for several reasons, including if you are pregnant, older or overweight.
Spilling is messy, but is not a disease and it is important that it is not treated or medicalised. The Americans call such infants the ‘happy spitters’.
Gastro-oesophageal reflux disease (GORD), however, is where the very acidic (pH 2) stomach contents reflux up, causing spilling, significant pain and irritability for a prolonged period of time after feeds. Other symptoms can include feed refusal, poor weight gain or arching of the back with feeds.
It is important to note that the natural history of reflux and GORD suggests a peak at three to four months of age, but resolution by six months in 60% of babies affected, and by 12 months in 98% of babies affected.
As there are no reliable tests for GORD (other than very specialised impedance studies involving a tube inserted into the oesophagus), the diagnosis is made on careful examination and consideration of other possible conditions that mimic GORD.
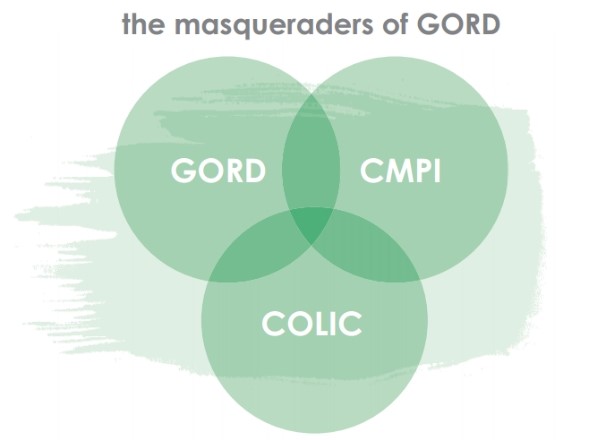
In disguise
Colic commonly masquerades as GORD. It is increasingly recognised that an altered gut microbiome (bacteria that live in our gut) is probably implicated in the development of colic and that some bacteria produce more gas, and therefore the symptoms of colic. Given that 50% of babies spill and a significant proportion have colic, it is easy to see how a baby with colic and spilling can be mistakenly diagnosed with having GORD. In these children, medication isn’t effective. By the time baby is four to six months of age, their colic will generally have resolved itself. Trials of probiotics to increase the proportion of good bacteria in the gut for the treatment of colic have mixed results, although larger trials have generally shown no benefit. More trial research is pending. The gut microbiome is an extremely topical area in medicine and considered widely at overseas conferences.
Another condition that can hide GORD is an intolerance to non-IgE mediated cow’s milk protein (CMPI). There are no blood, skin-prick or scientifically-validated hair analysis tests to diagnose this condition. It is due to a reaction to cow’s milk protein in the baby’s gut and occurs in 2-7% of babies, more commonly in those formula-fed than breast-fed. CMPI should be considered if babies with symptoms of reflux do not improve with medication, and particularly if they have lower GI symptoms. However, there is a lot of overlap with colic and spilling symptoms.
If a dairy exclusion is done and a baby has CMPI, there will be a marked improvement in symptoms in two weeks, however a re-trial of dairy products is always advised to ensure that symptoms haven’t just resolved coincidentally, as usually babies are around four to six months by this stage. This prevents mothers from excluding dairy from their diet, without proof of benefit, and also prevents formula-fed babies being on unnecessary medicalised formulas. The CMPI condition improves with time, usually by two to three years of age. It is important not to confuse this with IgE-mediated cow’s milk allergy, which presents with a sudden (within 30 minutes) acute reaction to dairy, such as facial rash and swelling of eyes. If breastfeeding mothers are on a dairy-free diet, it is very important they take calcium and vitamin D supplements to safe-guard their bone health.
My personal opinion is that the difference between colic and normal spilling, GORD and CMPI can be difficult to diagnose. My practice is to go through a careful examination and explanation of normal physiology, then begin a trial of a particular treatment and reassess it after two to four weeks.
Remember, most reflux symptoms in infants will generally improve with time. This is often why various practitioners claim success with their treatments, whereas the randomised double blind placebo controlled trials in medical literature are disappointing in demonstrating such treatment success, despite anecdotal reports to the contrary. This is true of both western and alternative approaches. While you may find relief with a particular treatment, you may simply find time to be the healer and the ancient proverb true also of reflux – “this too shall pass”
ALTERNATIVE REMEDIES
What you can try, when nothing else works:
■ Acupuncture/Acupressure Balances baby's energy and can calm the discomfort of irritation in the gut.
■ Chiropractic/Osteopathic care Spinal stress from childbirth can contribute to digestive disturbances. When this stress is alleviated there can be significant improvements in baby's comfort..
■ Probiotics Too much bad bacteria in the gut can make digestion a problem. Probiotics encourage heathy bacteria and restore balance to the gut.
■Baby massage Certain strokes can move milk and wind around the intestines to relieve pain. In the long term, muscles are toned which can also improve reflux.
■ Naturopathic remedies A naturopath can provide a wide range of therapies to aid digestion and relieve discomfort.
ALL IT TOOK WAS TIME
OHbaby! art director, Jaimee Clapham, shares her story.
If you had visited my house two and a half years ago, you would have been greeted by a tired new mother with an irritable newborn strapped to her front and asked to "please, excuse the floor", which resembled Muriwai Beach's Gannet Rock — dried-up white splotches everywhere. We gave up on bending down to mop up a spill every time it happened, as it happened constantly. Unfortunately, our little girl wasn't a 'happy spitter' and she was diagnosed with reflux at seven weeks old by a paediatrician. He prescribed her Gaviscon Infant and recommended for me to trial a dairy-free diet. Her father and his brother both had CMPI as littlies, so the suspicion of dairy in my diet had already been raised by my midwife during the first few troublesome weeks.
At the time of diagnosis, her symptoms seemed a bit like colic — a lot of inconsolable crying, wind issues and very short sleep cycles. Everyone was saying, "oh, she just has colic. She will grow out of it in a few months". However, where as colic is crying pretty much all day long, she only cried when lying flat in the pram, carseat and bassinet, or after being breastfed. On one occasion after a feed, she cried inconsolably for over an hour. I'll never forget the moment when she stopped crying, went as stiff as a board and froze breathless in my arms for about six seconds... then started crying again. Had my tiny eight-week-old baby just had a seizure? I called the paediatrician and explained what had happened. He assured me it wasn't a seizure, but in fact an adverse reaction to the pain she was experiencing.
Instead of that magical milk-drunk-baby effect that I had witnessed for the first three weeks of feeding, I now had a baby who was only happy and content before being fed. By four months old, she had developed a strange cough that only occurred after being fed, and then she finally refused feeds altogether; being held in a feeding position and the sight of me lifting up my top was enough to make her cry and turn away.
During the time of this 'breast aversion', I was having to make up for all missed (refused) feeds during the night. She would accept a feed during the night if she was half asleep, so I was dream-feeding her every three hours throughout the night for a week. During one day, I thought I would test both a bottle and soy formula to see if that made a difference. I was still wondering if she was lactose intolerant, as my dairy/gluten-free diet, and her now taking 5mg of omeprazole beads per day, weren't showing much effect. That day we learnt she is severely intolerant to soy, and ended up in Starship Hospital with a grey, limp four-month-old who had vomited over six times. I could now add 'soy-free' to my diet's repertoire.
By nine months old, our little girl was still very irritable and was only content when being distracted. However, the happy moments were often brief and she would occasionally, out of nowhere, fl are up into full-blown screaming, arching backwards or contorting into an s-shape when trying to console her.
Then came her first teeth. Even though her self-settling and night sleep had got much better since being on omeprazole, teething ruined everything! Most websites I read said that teething seemed to fl are up reflux symptoms and this was true for her. For a month we had her sleep in our bed every night to help her get through the cutting of her first teeth, which was exasperating the reflux pain. Most nights she would wake and scream and arch and twist her head for sometimes up to two hours. Nothing helped, she didn't even like to be cuddled. This is when I started giving her a teaspoon of Mylanta, and most of the time, this settled her within fi ve minutes. Seeing that an adult's antacid formula was remarkably settling her from this inconsolable state was probably the first time I truly realised she was most definitely experiencing GORD and heartburn and it wasn't from my milk or anything in her diet (she was also dairy/soy/gluten free).
During this tough month, our GP suggested upping her daily dose of omeprazole and giving her a dummy at bedtime. She said the sucking increases saliva production, which helps to naturally neutralise the stomach acid. After 10 days we really noticed a difference in her moods, behaviour and self-settling ability, and at eleven months old, she was sleeping through the night in her own cot. I had read, somewhere, that until you get the correct dose of medication sorted, it can be like they're on no meds at all. Once we found her magic dose, we saw a radical change, although we then faced a long and slow weaning process, with a few rebounds. But she was happily off medication by 20 months old.
Now, at two-and-a-half, little miss is a happy, healthy and thriving wee girl. She is still intolerant to soy, dairy and wheat and only stopped choking and coughing when drinking liquids six months ago. All these things help paint a picture as to why she may have had infantile GORD, but no one really has the answers as to why some are 'happy spitters' and some experience such awful discomfort. Just that, unfortunately, s*** happens.

AS FEATURED IN ISSUE 31 OF OHbaby! MAGAZINE. CHECK OUT OTHER ARTICLES IN THIS ISSUE BELOW















Cookie Policy | Terms & Conditions | Privacy policy | Copyright © 2026 www.ohbaby.co.nz. All Rights reserved.